What is a Hernia?
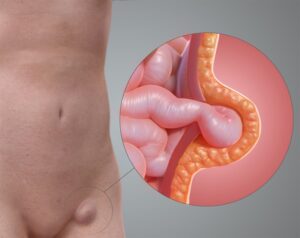
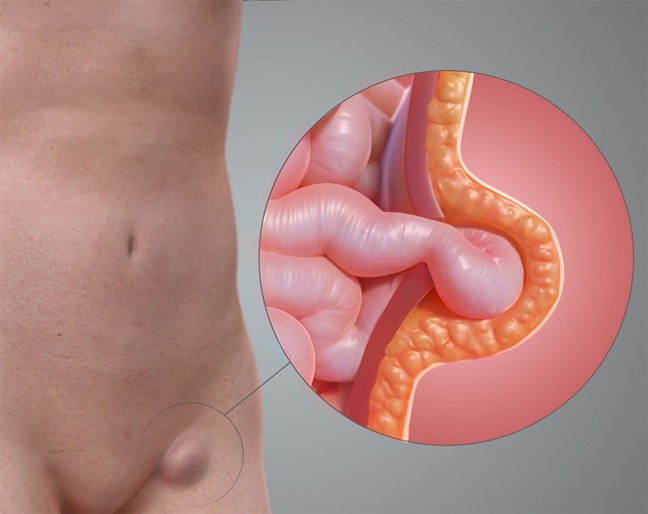
A hernia occurs when an organ or tissue pushes through a weak spot in the surrounding muscle or connective tissue. Hernias are most commonly found in the abdomen, but they can also appear in the upper thigh, belly button, and groin areas. While hernias are usually not life-threatening, they can cause discomfort and may require surgical intervention to prevent complications.
Common Types of Hernias
There are several common types of hernias, each with its unique characteristics and challenges:
Inguinal Hernia
Inguinal hernias occur when a part of the intestine or fat protrudes through the abdominal wall or into the inguinal canal in the groin. They are more common in men and can cause pain, especially when coughing, bending over, or lifting heavy objects.
Hiatal Hernia
A hiatal hernia occurs when part of the stomach pushes up through the diaphragm into the chest cavity. This type of hernia can cause acid reflux, heartburn, and chest pain.
Umbilical Hernia
Umbilical hernias occur near the belly button when part of the intestine protrudes through the abdominal wall. They are common in infants but can also affect adults, especially those who are overweight or have had multiple pregnancies.
Incisional Hernia
Incisional hernias occur at the site of a previous surgical incision. The intestines or other tissues push through the weakened area of the abdominal wall, causing a bulge.
Femoral Hernia
Femoral hernias occur when tissue pushes through the wall of the femoral canal in the upper thigh/near the groin. They are less common and more frequent in women, often presenting a higher risk of complications.
Ventral Hernia
A ventral hernia occurs when tissue bulges through an opening in the muscles of the abdomen. These can occur at any location on the abdominal wall.
Epigastric Hernia
Epigastric hernias occur between the belly button and the lower part of the ribcage in the midline of the abdomen. They can cause pain and discomfort, particularly when laughing, coughing, or straining.
Causes and Risk Factors
Understanding the causes and risk factors for hernias can help in prevention and management:
Straining and Heavy Lifting
Lifting heavy objects, straining during bowel movements, or intense coughing can increase the risk of developing a hernia by putting pressure on the abdominal wall.
Pregnancy
The increased pressure on the abdominal wall during pregnancy can lead to the development of hernias.
Obesity
Excess weight puts additional strain on the abdominal muscles, increasing the risk of hernias.
Previous Surgery
Past surgeries, especially those involving the abdomen, can weaken the abdominal wall and lead to incisional hernias.
Genetics
A family history of hernias can increase the likelihood of developing one.
Chronic Conditions
Chronic cough, constipation, and other conditions that increase abdominal pressure can contribute to the development of hernias.
Symptoms
Symptoms of hernias can vary depending on the type and severity but may include:
- A noticeable lump or bulge in the affected area may increase in size when standing or straining and disappear when lying down.
- Pain or discomfort at the hernia site, especially when bending over, coughing, or lifting. In the case of hiatal hernias, symptoms may include heartburn and chest pain.
- A feeling of weakness, heaviness, or pressure in the abdomen or groin.
- In severe cases, particularly with strangulated hernias, nausea and vomiting may occur.
- For hiatal hernias, difficulty swallowing (dysphagia) can be a symptom.
- In some cases, hernias can cause constipation or bowel obstruction, leading to severe pain and digestive issues.
Diagnosis
Accurate diagnosis of hernias is essential for effective treatment. Common diagnostic procedures include:
Physical Examination
A healthcare provider will examine the affected area for visible bulges and may ask you to cough or strain to detect the hernia.
Imaging Tests
Ultrasound, CT scans, and MRI scans help visualise the hernia, determine its size and location, and assess for complications such as bowel obstruction.
Endoscopy
For hiatal hernias, an endoscopy may be performed to visualize the inside of the esophagus and stomach and assess the extent of the hernia.
Treatment
Treatment for hernias varies depending on the type, size, and severity of the hernia. Common treatment options include:
- For small, asymptomatic hernias, a wait-and-see approach may be recommended, with regular monitoring by a healthcare provider.
- Diet – For hiatal hernias, dietary changes to reduce acid reflux, such as avoiding spicy foods, can be helpful.
- Weight Management – Losing weight can reduce abdominal pressure and alleviate symptoms.
- Antacids and Proton Pump Inhibitors – For hiatal hernias, these medications can help manage acid reflux and heartburn.
- Open Surgery – A surgical procedure where the hernia is repaired through a larger incision.
- Laparoscopic Surgery – A minimally invasive procedure using small incisions and a camera to guide the repair. This method typically has a shorter recovery time and less postoperative pain.
- Mesh Repair – Often used in both open and laparoscopic surgeries, a synthetic mesh is placed over the weakened area to provide additional support and prevent recurrence.
- Emergency Surgery – In cases where the hernia is causing severe pain, obstruction, or strangulation (cutting off blood supply to the affected tissue), emergency surgery is necessary to prevent serious complications.
Managing and Preventing Hernias
Effective management and prevention strategies can help minimise symptoms and reduce the risk of recurrence:
- Use proper lifting techniques and avoid lifting heavy objects to reduce strain on the abdominal muscles.
- Losing excess weight can reduce abdominal pressure and lower the risk of developing hernias.
- Engaging in exercises that strengthen the core muscles can provide additional support to the abdominal wall.
- Managing conditions that increase abdominal pressure can help prevent hernias.
- For those with existing hernias, wearing a supportive garment or hernia belt can help alleviate symptoms and prevent the hernia from worsening.